In our previous posts, we discussed the mathematical tools of evaluation—discrimination, calibration, and threshold selection. But these are not just abstract statistics for data scientists. They are the concrete evidence of an organization’s values.
How you evaluate an AI model directly reflects your strategic principles. If you measure only accuracy, you signal that you care about marketing. If you measure calibration and generalizability, you signal that you care about patient safety. To build a sustainable AI program, we must connect these technical metrics to the core pillars of healthcare governance.
Connection to Strategic Principles
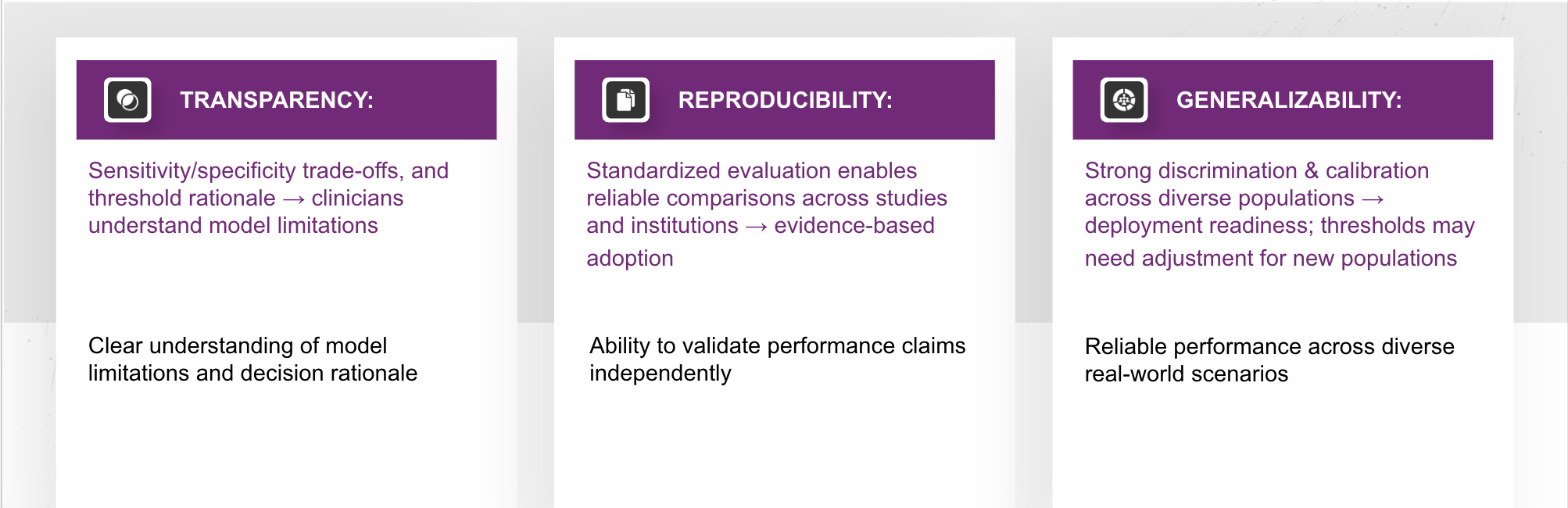
Rigorous evaluation measures directly support the three critical pillars of healthcare AI governance:
- Transparency: By explicitly stating trade-offs, AUC metrics, and threshold rationales, we help clinicians understand exactly what the model can (and cannot) do.
- Generalizability: Models that maintain strong discrimination and calibration across diverse datasets demonstrate they are actually ready for deployment, not just research.
- Reproducibility: Standardized evaluation protocols allow us to reliably compare results across different studies and institutions, eliminating the “black box” problem.
Strategic Implication:
Healthcare organizations must evaluate AI systems using comprehensive frameworks—including discrimination, calibration, and clinically appropriate thresholds. Any reported performance metrics require scrutiny to ensure they are not just mathematically high, but clinically relevant.
How Evaluation Measures Expose Framework Weaknesses
When these evaluation principles are ignored, the cracks in the framework become visible. We can see this in three specific areas:
1. Transparency Gaps
Without clear threshold selection, sensitivity and specificity values lose their meaning. If a vendor cannot explain why a specific threshold was chosen, or lacks data transparency, it prevents the clinical team from understanding if the calibration is reliable.
2. Reproducibility Failures (The DeepMind Lesson)
A notable example occurred with a Google DeepMind kidney injury model. While promising, the lack of transparency created significant hurdles:
- Inconsistent Results: Independent re-creations of the model produced inconsistent AUCs.
- Hidden Thresholds: A lack of threshold visibility led to uncertainty about the true performance gaps.
- Code Opacity: Missing evaluation code made independent calibration assessment impossible.
3. Generalizability Problems
This is the most dangerous failure mode for patient care. When evaluation is weak, we see:
- AUC Variation: Performance that drops from near-perfect to random chance when moving between hospitals.
- Calibration Drift: A model might preserve its ranking ability (discrimination) but lose its accuracy on probability (calibration).
- Threshold Failure: Tuning a model for one population may cause it to fail catastrophically in another.
The Cascade Effect
These are not isolated issues; they are interconnected risks. A weakness in one area triggers a chain reaction that destabilizes the entire AI program:
- Transparency Gaps $\rightarrow$ Lead to unclear evaluation $\rightarrow$ Which results in Unreproducible Claims.
- Reproducibility Issues $\rightarrow$ Lead to inconsistent results $\rightarrow$ Which creates Uncertain Generalizability.
- Generalizability Issues $\rightarrow$ Lead to unstable performance $\rightarrow$ Which results in Unreliable Decision Support.
Conclusion: Governance is Built on Math
The lesson for oncology leaders is clear: Governance is not just a document signed in a boardroom. It is enforced in the code and the calculations.
By insisting on comprehensive evaluation—looking for calibration drift, demanding reproducibility, and scrutinizing transparency—we stop “The Cascade Effect” before it starts. This is how we move from buying “magic box” AI solutions to building a resilient, accountable infrastructure that improves patient outcomes for the long term.
Authored By: Padmasri Bhetanabhotla